Case Reports (SJCR)
Stechnolock Journal of Case Reports
Full Text
Volume 2, Issue 1
Giant Retroperitoneal Liposarcoma: Case Report
*Corresponding Author: Abraham Ariaya, St. Paul's Hospital Millennium Medical College, Medical school in Addis Ababa, Ethiopia, Tel: +251961016194, E-mail: abraham.ariaya@gmail.com
doi: /sjcr.2021.2.104
Citation: Mahteme Bekele, Tsega Terefea, Abraham Ariaya (2022) Giant Retroperitoneal Liposarcoma: Case Report. Stechnolock J Case Rep 2: 1-6
Copyright: © 2022 Abraham Ariaya. This is an open-access article distributed under the terms of Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.


Abstract
Liposarcomas are mesenchymal slow growing tumors of mesodermal origin with different subtypes: liposarcoma (41%), leiomyosarcoma (28%), malignant fibrous hisiocytoma (7%), fibrosarcoma (6%) and tumors of peripheral nerve sheath (3%.) liposarcomas can present in various locations such as the extremities, trumk, head, neck, mediastinum and retroperitoneum. The peak incidence is in the age group of 50-70 years. Liposarcoma is the most frequent histopathological variety of the retroperitoneum. Retroperitoneal sarcomas account for 15% of all sarcomas. [1-3]
Retroperitoneal liposarcomas alone comprise 0.07-0.2% of all neoplasias, 85% of these are malignant. Well differentiated liposarcomas are the most common histological subtypes encountered [1, 2]
Due to its deep location it causes adjacent organ compromise in upto 80% of cases. Patients usually present late because such tumors arise in large potential spaces of the retroperitoneum and can grow to large sizes without producing symptoms. Liposarcomas above 20kg are called “Giant Liposarcomas” and are extremely rare. The mainstay of management of liposarcoma is surgery, with retroperitoneal liposarcomas requiring a more aggressive surgical approach. [1,4,5]
In this study we report the case of a giant retroperitoneal liposarcoma that was successfully surgically excised.
Keywords: Giant Hernia; Sliding Hernia; Abdominal Compartment Syndrome
Case Discussion
A 60 years old male patient presented with a 2-year complaint of abdominal swelling with associated loss of appetite, constipation of 1 year and easy fatiguability of 4 months duration. He was treated at a private hospital with the presumptive diagnosis of lymphoma with CHOP regimen and took 3 cycles of chemotherapy with the last cycle taken 6 weeks prior to presentation to our hospital. Otherwise, he had no other complaints and had stable vital signs.
On physical examination he had a hugely distended abdomen with a palpable mass occupying the entire abdomen.
Investigation: CBC, LFT and RFT variables were within normal range. US was suggestive of a large intra-abdominal echogenic mass lesion having mass effect on bowel loops which are displaced laterally. suggestive of liposarcoma with right side mild hydronephrosis. US guided FNAC: atypical lipomatous tumor suggestive of well differentiated liposarcoma.
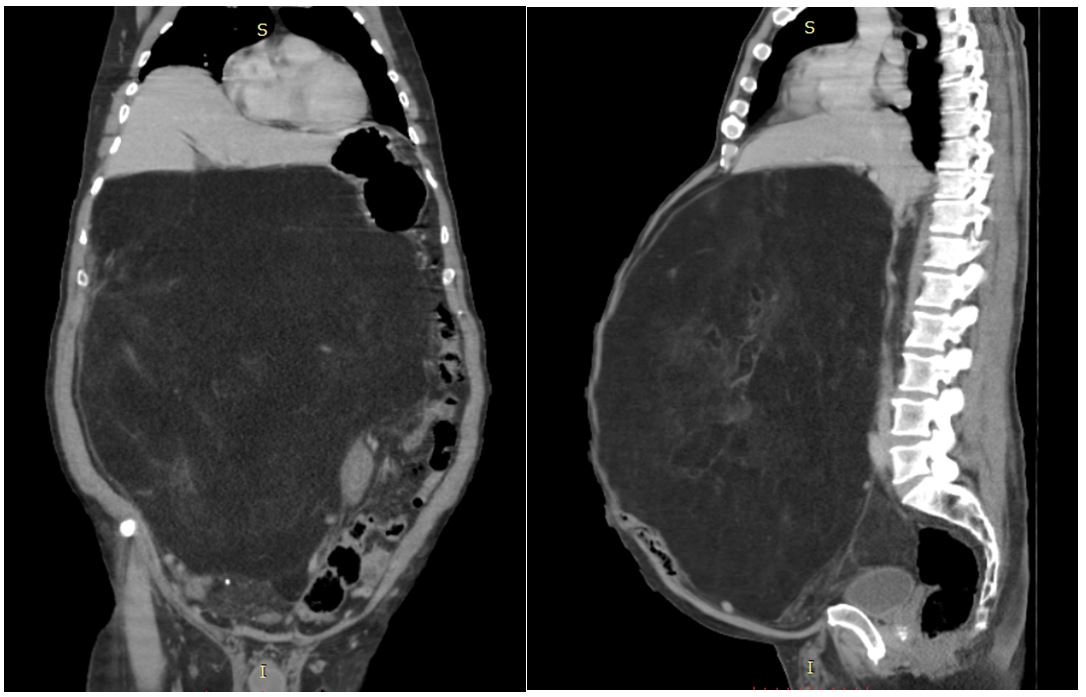
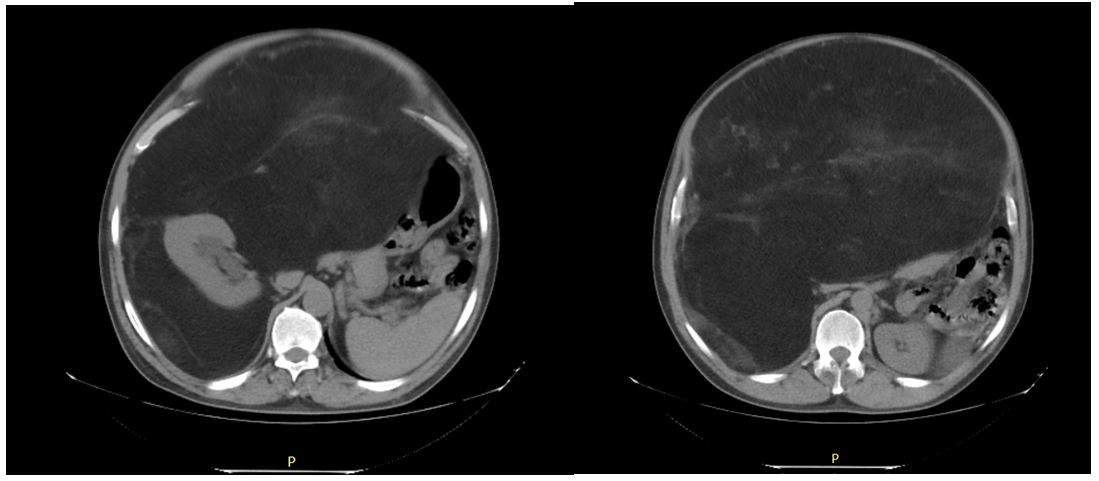
CT with contrast was done and showed a huge fat containing right retroperitoneal mass measuring 42x33x32 cm with an enhancing component. The mass was encasing around the kidneys with obstruction of the right PUJ having mild hydronephrosis. The mass displaces bowel and retroperitoneal vessels.
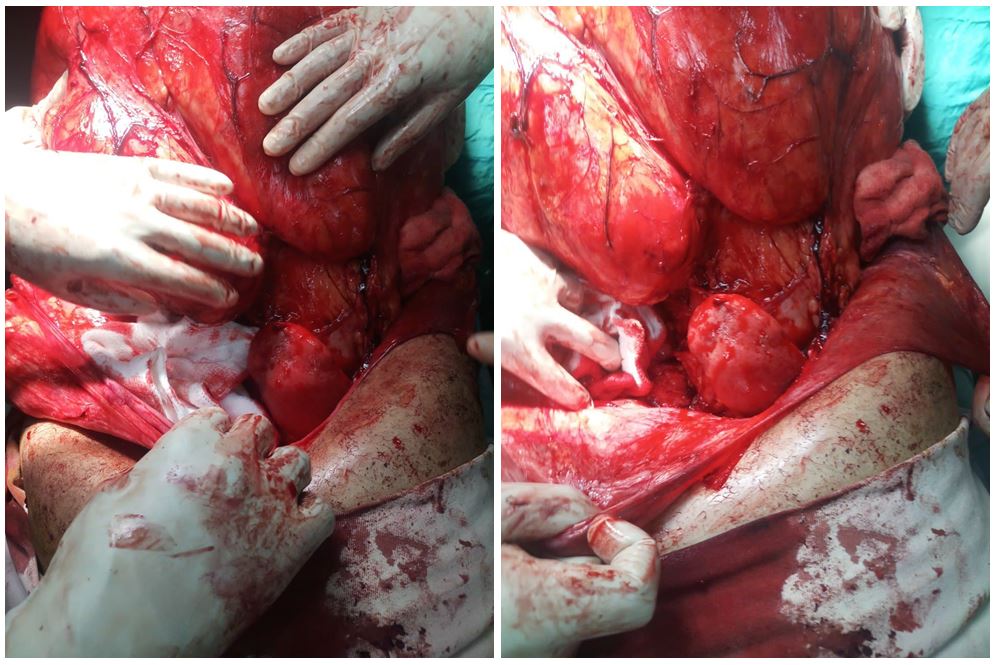
Operative findings: under general anesthesia the abdomen was approached through a midline vertical incision and a huge right retroperitoneal mass had displaced the cecum and ascending colon.
The right kidney was displaced upwards and surrounded by the mass but not invaded. The retroperitoneum was entered posterior to the mass and the mass was mobilized. The right renal vessels and ureter were isolated and spared and the mass was inoculated and a drain was left and retroperitoneum subsequently closed.
The specimen was sent for pathology and patient was taken to the recovery with stable vital signs.
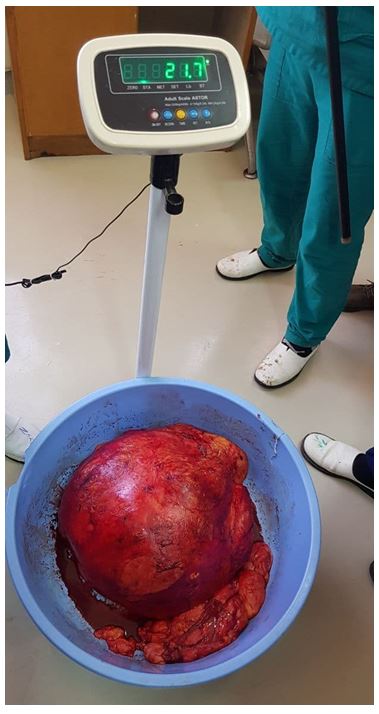
The mass (Pictured) was then weighed and found to be 21.7kg. The patient was discharged on his 5th post-op day and has had an uneventful follow up at our referral clinic. The pathology report came back as a well differentiated liposarcoma.
Discussion
Liposarcomas are the most common histological type of retroperitoneal sarcomas. Liposarcomas occur most commonly in the extremities (52%), retroperitoneum (19%), and inguinal region (12%).
Those above 20kg are considered to be giant, but this finding is rare. 20% of liposarcomas are >10cm at the time of diagnosis. Up to 78% of cases present with a painless abdominal mass. Their mot common manifestations are nonspecific abdominal pain and a palpable abdominal mass. [1.2,3]
The preferred diagnostic methods are USG, CT and MRI which aid in the diagnosis and establishing the relation of the mass with neighboring organs. [3,5]
Patrik et al. demonstrated that in liposarcomas >10cm, complete resection can be carried out in upto 70% of cases. However, in upto 50% of these cases multiorgan resection is necessary in order to reach this goal. [1,3] The most frequent organ resected is the kidney (30%) [1,2,4] preoperative bowel preparation is advised. The most common serious postoperative complications are hemorrhage and anastomotic leakage from bowel resection. [3] Our case was 42cm at its widest dimension and weighed 21.7kg and we were able to spare the right kidney during resection.
Liposarcomas are localy aggressive and have high recurrence rate upto 40-80% but distant metastasis is rare. [3,5] Mesodermic tumors are radioresistant, but liposarcoma is more radiosensitive. But the place of post surgical radiotherapy has been debated among different authors. [1,2,4] Chemotherapy does not improve survival or the likelihood of metastasis. [3]
Conclusion
Giant retroperitoneal liposarcomas are rare findings which can pose challenges to the surgeon due to their massive size and associated local invasion. Complete surgical resection is the treatment of choice.
Competing Interests
The authors declare that they have no competing interests
Consent
Written informed consent was obtained
- Ángel Herrera-Gómez et al. (2008) Giant retroperitoneal liposarcoma, World J Surg Oncol 6:115
- Chavan Shahaji et al. (2012) Giant Retroperitoneal Liposarcoma: A Case Report, Case Rep in Oncol Med 8: 869409
- Antonio Morandeira et al. (2008) Giant retroperitoneal sarcoma, Can J Surg 51: 79-80
- Isaac R Francis et al. (2005) Retroperitoneal sarcomas, Cancer Imaging 5: 89-94.
- Rikki Singal et al., (2018) A giant retroperitoneal sarcoma: current pathology and successful surgically, Acta Gastroenterol Latinoam 48: 52-5